Become a Patient












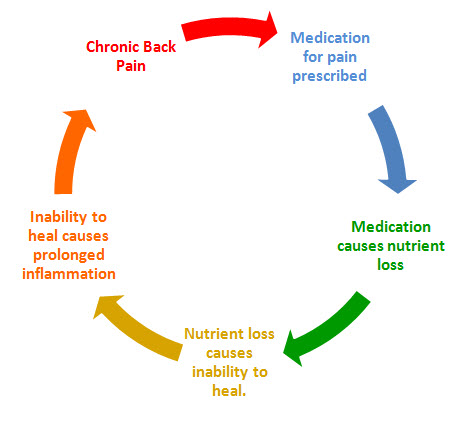 Pain Medications Cause Joint Pain & Joint Damage
Pain Medications Cause Joint Pain & Joint Damage
Back pain is the second most common condition that people visit their doctor for. Likewise, prescriptions medications to treat pain are often the first line o treatment recommended by doctors. Unfortunately, pain medications do little to address the actual origin of the pain and serve more to mask the outward symptoms. The consequences of long […]
 Dr. Osborne and Gluten Free Society Host Holiday Meeting
Dr. Osborne and Gluten Free Society Host Holiday Meeting
How To Navigate the Holidays and Stay on a Gluten Free Diet Make sure you save the date. When? Saturday, November 2nd, 2013 Where? University Branch Library Address – 14010 University Blvd. – Sugar Land, TX 77479 (At the University of Houston Sugar Land Campus). Map it here <<< Time? 11:00 am – 1:00 pm […]

